Fill Out a Valid DD 2870 Form
The DD 2870 form is an essential document used primarily by military personnel and their families to request medical treatment or services. This form plays a crucial role in ensuring that service members have access to the healthcare benefits they are entitled to under various military health programs. It captures vital information about the individual seeking care, including personal details, medical history, and the specific services being requested. By filling out the DD 2870, users can streamline their healthcare experience, making it easier for healthcare providers to understand their needs. Additionally, this form is significant for maintaining accurate records within the military healthcare system, which is vital for both administrative purposes and the effective delivery of care. Understanding how to properly complete and submit the DD 2870 can greatly enhance the efficiency of accessing necessary medical services, ultimately supporting the health and well-being of those who serve in the armed forces and their dependents.
Common mistakes
When filling out the DD 2870 form, many individuals encounter common pitfalls. Below is a list of mistakes that people often make, which can lead to delays or complications in processing their requests.
- Incomplete Information: Many forget to fill in all required fields, which can result in the form being returned or delayed.
- Incorrect Identification: Using the wrong identification number or failing to provide one can hinder the processing of the request.
- Missing Signatures: Some individuals neglect to sign the form, which is crucial for validation.
- Not Providing Supporting Documents: Failing to attach necessary documents can lead to further complications.
- Using Outdated Versions: Submitting an old version of the form can cause delays, as only the most current version is accepted.
- Incorrect Mailing Address: Providing an incorrect address can result in lost forms or delays in communication.
- Ignoring Instructions: Many overlook the detailed instructions that accompany the form, leading to errors.
- Neglecting to Keep Copies: Failing to keep a copy of the submitted form can be problematic if there are questions or issues later.
- Rushing the Process: Taking time to carefully review the form before submission can prevent many of these mistakes.
By being aware of these common mistakes, individuals can improve their chances of a smooth and efficient process when completing the DD 2870 form.
Preview - DD 2870 Form
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
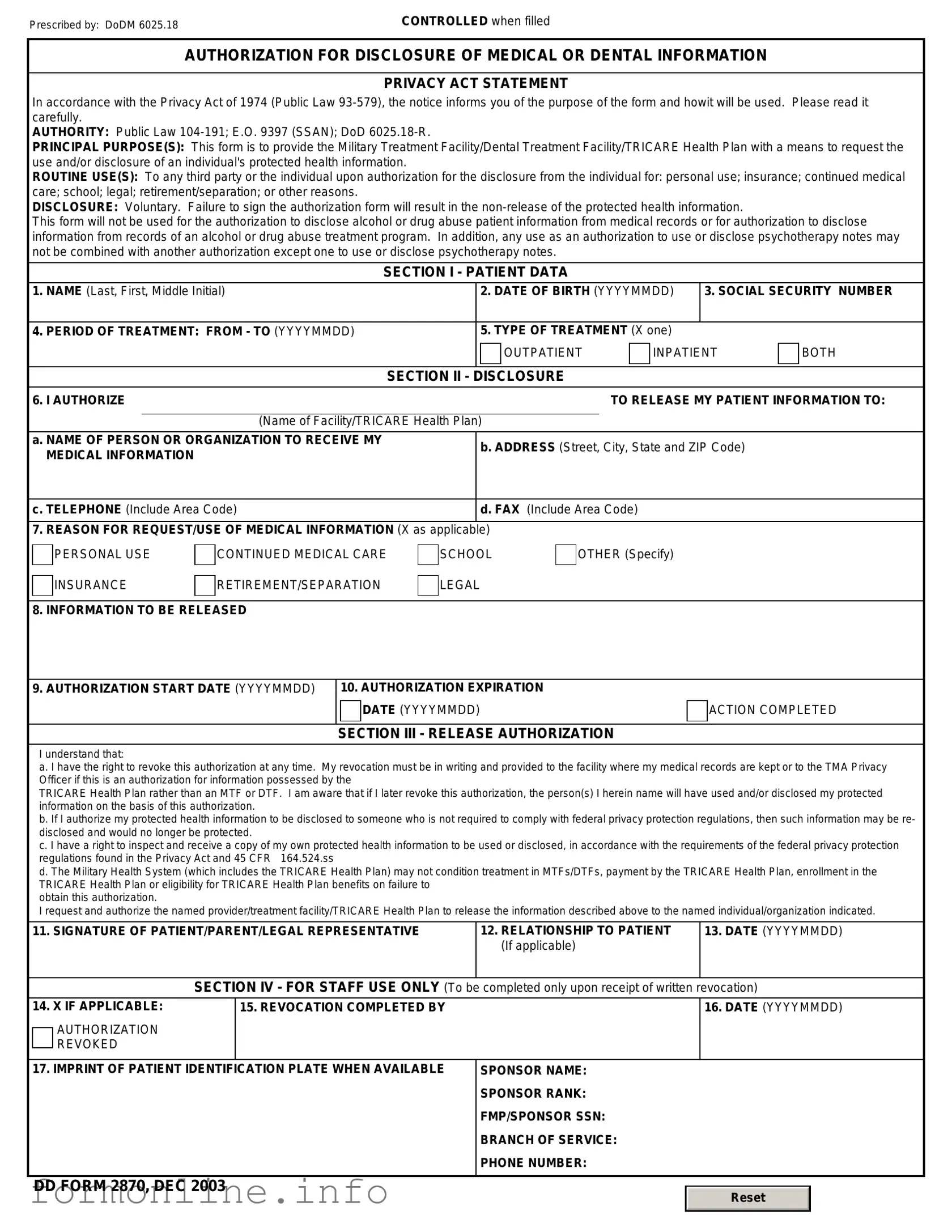
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Other PDF Templates
Can I9 Be Signed Electronically - Complete and accurate I-9 forms contribute to a lawful workforce and protect against identity theft.
The Texas Mobile Home Bill of Sale serves as a vital legal instrument that ensures the ownership of a mobile home is transferred properly between parties, covering essential information such as the buyer's and seller's details, the mobile home's characteristics, and the agreed sale price. For those looking to navigate this process effectively, the Mobile Home Bill of Sale can provide clarity and guidance, helping to protect the interests of everyone involved.
Irs Form 433 F Allowable Expenses - Understanding the 433-F can help you effectively manage tax liabilities.
Documents used along the form
The DD 2870 form is a critical document used in various military and veteran-related processes. It often accompanies several other forms and documents that help facilitate the necessary procedures. Below is a list of related documents that are commonly used alongside the DD 2870.
- DD Form 214: This document serves as a Certificate of Release or Discharge from Active Duty. It provides a summary of a service member's military career, including dates of service and type of discharge.
- SF 180: The Standard Form 180 is used to request military records from the National Personnel Records Center. It helps individuals obtain copies of their service records, which may be necessary for various applications.
- VA Form 21-526EZ: This form is used to apply for disability compensation and related benefits through the Department of Veterans Affairs. It streamlines the application process for veterans seeking assistance.
- ST-12B Georgia form - This form acts as a Purchaser’s Claim for Sales Tax Refund Affidavit, allowing individuals and businesses to formally request a refund of sales tax paid on eligible purchases; for more details, visit https://georgiapdf.com.
- DD Form 1172-2: This form is utilized to apply for a Uniformed Services Identification Card. It is essential for accessing military benefits and services.
- VA Form 22-1990: This form is used to apply for education benefits under the GI Bill. It assists veterans in accessing funding for educational programs and training.
These documents collectively support service members and veterans in navigating their rights and benefits. Proper completion and submission of these forms can significantly impact the efficiency of the application processes involved.
Similar forms
The DD Form 2870, known as the Authorization for Disclosure of Medical or Dental Information, is similar to the HIPAA Release Form. Both documents allow individuals to authorize the release of their medical records. The HIPAA Release Form is specifically designed to comply with the Health Insurance Portability and Accountability Act, ensuring that patient information is shared in a manner that protects privacy. Like the DD 2870, it requires the signature of the individual granting permission for their information to be disclosed.
One key document related to estate planning is the Florida Last Will and Testament form guide, which enables individuals to clearly outline their wishes for asset distribution following their passing. This form provides the necessary framework to ensure that beneficiaries and guardianship decisions align with the individual's intentions, offering peace of mind during a challenging time. For more information, refer to the Florida Last Will and Testament.
Another document comparable to the DD 2870 is the Medical Records Release Form. This form is commonly used by healthcare providers to obtain consent from patients before releasing their medical records to third parties. Similar to the DD 2870, it outlines what information can be shared, with whom, and for what purpose, ensuring transparency and patient control over their personal health information.
The Patient Authorization Form also shares similarities with the DD 2870. This form is used by various healthcare facilities to gain consent from patients for the use and disclosure of their health information. It typically specifies the information being released and the duration of the authorization, mirroring the structure and intent of the DD 2870.
The Release of Information Form is another document that resembles the DD 2870. This form is often utilized by hospitals and clinics to authorize the sharing of patient information with insurance companies or other healthcare providers. Like the DD 2870, it requires the patient’s consent and outlines the specifics of the information being disclosed.
The Consent to Treat Form is somewhat similar, as it also involves patient authorization. While primarily focused on granting permission for medical treatment, it often includes provisions for sharing medical information necessary for treatment purposes. This overlaps with the intent of the DD 2870, which is to facilitate the sharing of medical information.
The Release of Liability Form can be compared to the DD 2870 in terms of consent. This form is typically used in situations where individuals agree to waive certain rights, often in exchange for services. While it does not focus solely on medical information, it requires clear consent from the individual, similar to the process outlined in the DD 2870.
The Authorization for Use or Disclosure of Health Information Form is another document that aligns with the DD 2870. This form allows individuals to specify who can access their health information and under what circumstances. It serves the same purpose as the DD 2870 in ensuring that individuals have control over their medical records.
The Consent for Release of Information Form is also comparable. This document is commonly used in mental health settings to obtain consent for sharing sensitive information. Like the DD 2870, it emphasizes the importance of patient consent and outlines the specific information that can be disclosed.
Lastly, the Durable Power of Attorney for Healthcare is similar in that it allows individuals to designate someone to make healthcare decisions on their behalf. While it serves a broader purpose, it can include the authority to access medical records, aligning with the intent of the DD 2870 to facilitate the sharing of medical information with authorized individuals.
Dos and Don'ts
When filling out the DD 2870 form, it's important to follow specific guidelines to ensure accuracy and compliance. Here is a list of things to do and avoid:
- Do read the instructions carefully before starting.
- Do use black or blue ink to fill out the form.
- Do provide accurate and complete information.
- Do sign and date the form where required.
- Don't leave any required fields blank.
- Don't use correction fluid or tape on the form.
- Don't submit the form without reviewing it for errors.
- Don't forget to keep a copy of the completed form for your records.
Key takeaways
The DD 2870 form is an important document used primarily for the release of medical information. Here are some key takeaways to keep in mind when filling out and using this form:
- The form is used to authorize the release of medical records and information from military treatment facilities.
- Make sure to provide accurate and complete information to avoid delays in processing.
- Signature and date are required on the form to validate the request.
- It is essential to specify the duration for which the authorization is valid.
- Understand that you can revoke the authorization at any time by submitting a written request.
- Keep a copy of the completed form for your records.
- Contact the facility where the records are held if you have questions about the submission process.
Using the DD 2870 form correctly ensures that you can access necessary medical information efficiently. Always double-check your entries for accuracy.
How to Use DD 2870
Once you have the DD 2870 form ready, you will need to complete it accurately to ensure that your request is processed efficiently. Follow these steps carefully to fill out the form correctly.
- Begin by entering your personal information in the designated fields. This includes your full name, address, and contact information.
- Provide your Social Security Number (SSN) in the appropriate section.
- Indicate your relationship to the service member if applicable. This could be a spouse, child, or other dependent.
- Fill in the details of the service member, including their name, branch of service, and any relevant identification numbers.
- Clearly state the purpose of your request in the specified area on the form.
- Review the form for any errors or missing information. Ensure that all sections are completed.
- Sign and date the form at the bottom. This is crucial for validating your request.
- Make a copy of the completed form for your records before submitting it.
After filling out the form, it should be submitted to the appropriate office as indicated in the instructions provided with the form. Ensure that you follow any additional guidelines for submission to avoid delays in processing your request.