Fill Out a Valid Hospital Bill Form
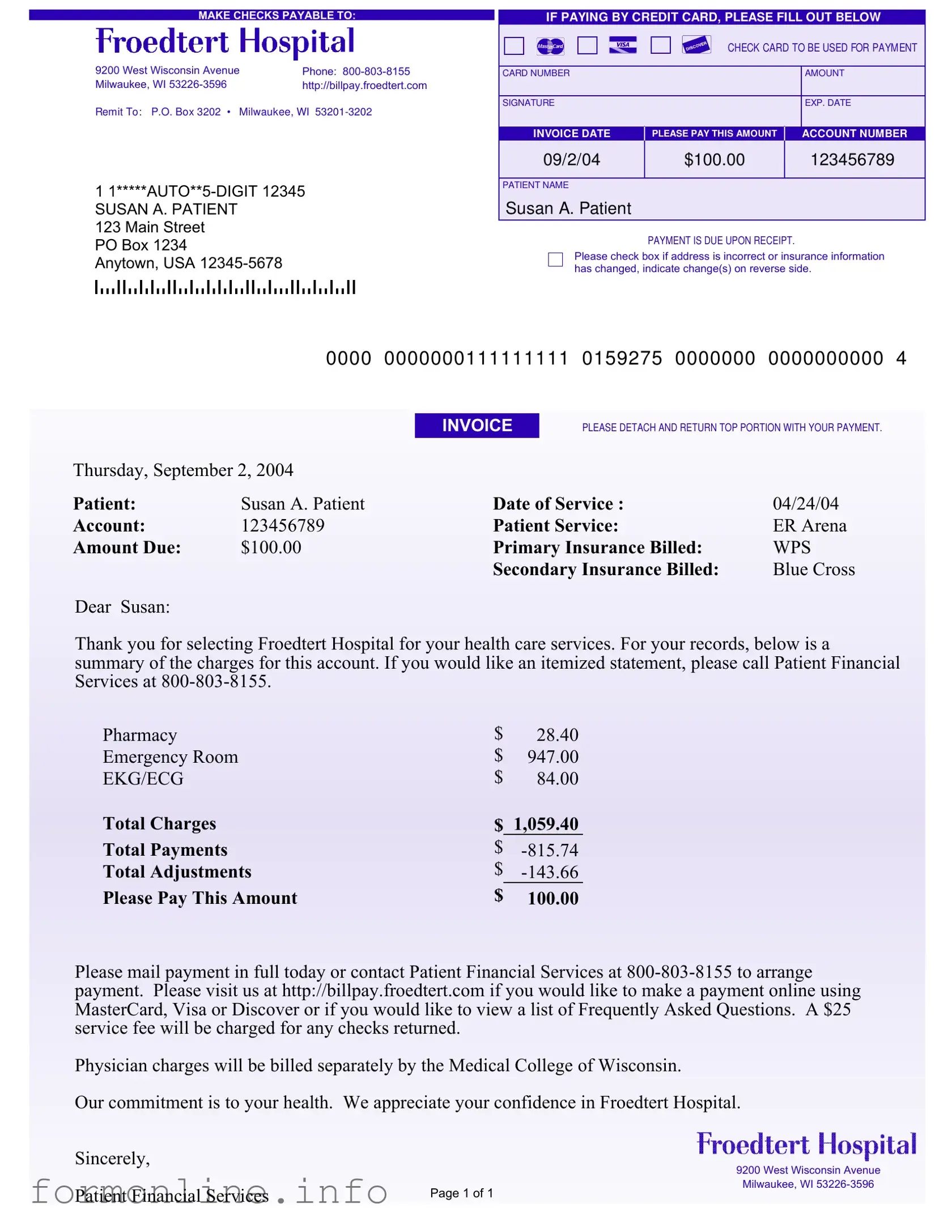
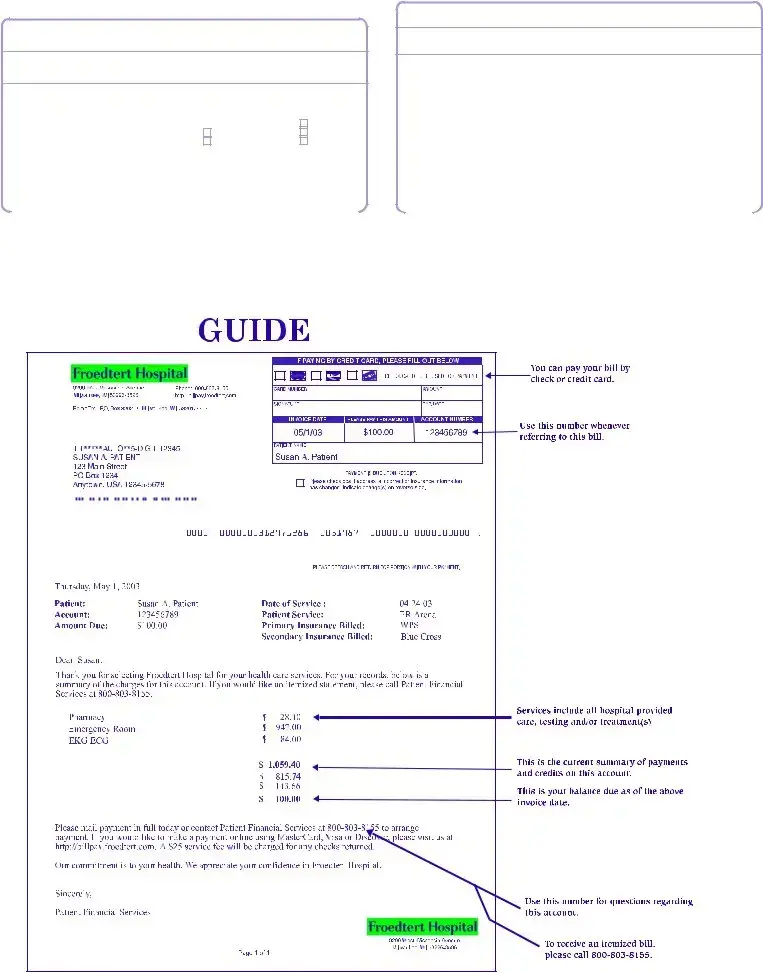
The Hospital Bill form is a critical document that provides patients with a clear overview of their medical expenses following treatment. It includes essential details such as the patient's name, service date, account number, and the total amount due. In addition to summarizing charges for services rendered, it lists payments and adjustments, giving patients a comprehensive view of their financial responsibilities. The form also highlights the importance of timely payment, indicating that the amount is due upon receipt. For those paying by credit card, specific fields are provided to ensure secure transactions. Patients are encouraged to contact Patient Financial Services for any inquiries regarding their bill or to request an itemized statement. Moreover, the form includes sections for updating personal and insurance information, ensuring that the hospital has accurate records. This attention to detail not only facilitates efficient billing but also fosters a transparent relationship between the hospital and its patients, emphasizing the institution's commitment to their health and financial well-being.
Common mistakes
-
Omitting Personal Information: Many individuals fail to provide complete personal details, such as their full name, address, or phone number. This can lead to delays in processing the bill.
-
Incorrect Insurance Information: Providing outdated or incorrect insurance details is a common error. This can result in the bill being sent to the wrong insurance provider, complicating payment.
-
Not Checking Payment Amount: Some people do not verify the total amount due before submitting payment. This can lead to overpayment or underpayment, causing further complications.
-
Ignoring Payment Methods: Failing to select the appropriate payment method can create confusion. If paying by credit card, it is essential to fill out the card information accurately.
-
Forgetting to Sign: A signature is often required for credit card payments. Neglecting to sign the form can result in the payment being rejected.
-
Not Updating Changes: When there are changes to personal or insurance information, individuals sometimes forget to update this on the form. This can lead to miscommunication and delays in processing.
-
Failing to Detach the Payment Portion: Some individuals overlook the instruction to detach the top portion of the bill before mailing. This can result in the payment being misdirected or lost.
Preview - Hospital Bill Form
MAKE CHECKS PAYABLE TO:
9200 West Wisconsin Avenue |
Phone: |
Milwaukee, WI |
http://billpay.froedtert.com |
Remit To: P.O. Box 3202 • Milwaukee, WI
1
SUSAN A. PATIENT
123 Main Street
PO Box 1234
Anytown, USA
IF PAYING BY CREDIT CARD, PLEASE FILL OUT BELOW
CHECK CARD TO BE USED FOR PAYM ENT
CARD NUMBER |
AMOUNT |
|
|
SIGNATURE |
EXP. DATE |
|
|
INVOICE DATE |
PLEASE PAY THIS AMOUNT |
ACCOUNT NUMBER |
09/2/04 |
$100.00 |
123456789 |
|
|
|
PATIENT NAME
Susan A. Patient
PAYMENT IS DUE UPON RECEIPT.
Please check box if address is incorrect or insurance information has changed, indicate change(s) on reverse side.
|
0000 |
0000000111111111 |
0159275 |
0000000 |
0000000000 |
4 |
|
|
INVOICE |
PLEASE DETACH AND RETURN TOP PORTION WITH YOUR PAYMENT. |
|
||
Thursday, September 2, 2004 |
|
|
|
|
|
|
Patient: |
Susan A. Patient |
Date of Service : |
|
04/24/04 |
|
|
Account: |
123456789 |
Patient Service: |
|
ER Arena |
|
|
Amount Due: |
$100.00 |
Primary Insurance Billed: |
WPS |
|
||
|
|
Secondary Insurance Billed: |
Blue Cross |
|
||
Dear Susan:
Thank you for selecting Froedtert Hospital for your health care services. For your records, below is a summary of the charges for this account. If you would like an itemized statement, please call Patient Financial Services at
Pharmacy |
$ |
28.40 |
Emergency Room |
$ |
947.00 |
EKG/ECG |
$ |
84.00 |
Total Charges |
$ |
1,059.40 |
Total Payments |
$ |
|
Total Adjustments |
$ |
|
Please Pay This Amount |
$ |
100.00 |
Please mail payment in full today or contact Patient Financial Services at
Physician charges will be billed separately by the Medical College of Wisconsin.
Our commitment is to your health. We appreciate your confidence in Froedtert Hospital.
Sincerely,
9200 West Wisconsin Avenue
|
Milwaukee, WI |
Patient Financial Services |
Page 1 of 1 |
|
PLEASE UPDATE ANY INFORM ATION THAT HAS CHANGED SINCE YOUR LAST STATEM ENT
ABOUT YOU:
YOUR NAME (Last, First, Middle Initial)
ADDRESS
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
|
|
|
|
|
|
|
MARITAL STATUS |
|
|
|
|
Separated |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
|
Divorced |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
Widowed |
|
||||||
EMPLOYER'S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER'S ADDRESS |
|
|
|
|
|
|
|
CITY |
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ABOUT YOUR INSURANCE:
YOUR PRIMARY INSURANCE COMPANY'S NAME
PRIMARY INSURANCE COMPANY'S ADDRESS
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
YOUR SECONDARY INSURANCE COMPANY'S NAME |
|
|
|
|
|
|
|
|
|
SECONDARY INSURANCE COMPANY'S ADDRESS |
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
Other PDF Templates
W9 Form 2022 - Tax identification numbers can be Social Security numbers or EINs.
Can I Leave a Note for Fedex Signature Required - Avoid delays by filling out the release form in advance of your delivery date.
The New York Mobile Home Bill of Sale is an essential legal document that facilitates the transfer of ownership of a mobile home, providing a clear outline of the transaction details including buyer and seller information, the mobile home's description, and the sale price. For a comprehensive understanding of this critical form, it is advisable to refer to the Mobile Home Bill of Sale to avoid any ambiguities and ensure both parties are protected during the sale.
Vehicle Vessel Transfer and Reassignment Form - This form supports requests for legal name changes linked to vehicle ownership.
Documents used along the form
When dealing with hospital bills, several other forms and documents often come into play. Understanding these documents can help ensure that you manage your medical expenses effectively. Here’s a brief overview of some commonly used forms alongside the Hospital Bill form.
- Insurance Claim Form: This form is submitted to your insurance company to request reimbursement for medical expenses. It includes details about the services received, the costs, and the patient’s insurance information.
- Power of Attorney Form: This document is important for granting someone authority to make decisions on your behalf in critical situations. For more details, visit https://georgiapdf.com/.
- Itemized Statement: An itemized statement provides a detailed breakdown of charges incurred during your hospital visit. It lists each service, its cost, and any payments or adjustments made. You can request this from the hospital if you need clarification on your bill.
- Patient Registration Form: This document collects essential information about the patient, including personal details, insurance information, and medical history. It is typically filled out during the initial visit to the hospital.
- Payment Plan Agreement: If you cannot pay your bill in full, this agreement outlines a plan to pay in installments. It specifies the payment amount, due dates, and any interest or fees associated with the plan.
- Financial Assistance Application: Many hospitals offer financial aid for those who qualify. This application helps determine your eligibility for assistance based on income, family size, and medical expenses.
Understanding these documents can simplify the billing process and help you navigate your healthcare expenses. Always keep copies of your forms and any correspondence related to your hospital bills for your records.
Similar forms
The first document similar to the Hospital Bill form is the Medical Invoice. This document outlines the services provided to a patient, along with the associated costs. Like the Hospital Bill, it specifies the total amount due, payment options, and details about insurance coverage. Both documents serve the purpose of informing patients about their financial responsibilities after receiving medical care.
An Insurance Claim Form is another document that shares similarities with the Hospital Bill form. This form is used to request payment from an insurance company for medical services rendered. It includes information about the patient, the provider, and the services provided. Just as the Hospital Bill provides a summary of charges, the Insurance Claim Form details the same services but focuses on obtaining reimbursement from the insurer.
The Patient Statement is yet another comparable document. This statement provides a summary of a patient's account, including charges, payments, and any outstanding balance. Similar to the Hospital Bill, it serves as a reminder of what is owed and may include instructions for payment. Both documents aim to keep patients informed about their financial obligations regarding their healthcare.
A Prescription Bill is also related to the Hospital Bill form. This document details the costs associated with medications prescribed to a patient. Like the Hospital Bill, it includes information about the patient and the total amount due for the medications. Both documents emphasize the importance of timely payment for services rendered.
The Explanation of Benefits (EOB) is another document that bears resemblance to the Hospital Bill. The EOB is sent by an insurance company after a claim has been processed. It explains what services were covered, the amount billed, and the patient's financial responsibility. Much like the Hospital Bill, it provides clarity on what the patient owes after insurance has contributed.
A Payment Plan Agreement is similar in that it outlines the terms under which a patient can pay their medical bills over time. This document details the payment amounts, due dates, and total balance owed. Like the Hospital Bill, it is essential for managing financial obligations and ensuring that patients understand their payment responsibilities.
An Itemized Bill is closely related to the Hospital Bill form as well. This document breaks down each service provided, along with its corresponding cost. It offers a more detailed view of charges, similar to the summary provided in the Hospital Bill. Patients can use both documents to understand their financial situation better.
The Balance Due Notice is another document that resembles the Hospital Bill. This notice is typically sent to remind patients of any outstanding balances. It includes the total amount due and may provide payment options. Like the Hospital Bill, it serves as a prompt for patients to settle their accounts.
In addition to the documents mentioned above, understanding the role of the Ohio Motor Vehicle Bill of Sale form is essential for those involved in vehicle transactions. This form, necessary for the legal transfer of ownership, can be accessed at autobillofsaleform.com/ohio-motor-vehicle-bill-of-sale-form/, ensuring that buyers and sellers are aware of their rights and responsibilities during the sale process.
A Financial Assistance Application is also comparable to the Hospital Bill form. This document allows patients to apply for financial aid to help cover medical expenses. It requires similar information about the patient’s financial situation and insurance coverage. Both documents are aimed at ensuring that patients receive the care they need without undue financial burden.
Finally, a Collection Notice is similar in that it communicates the need for payment on overdue accounts. This document is often sent when payments are significantly past due. Like the Hospital Bill, it outlines the amount owed and may include options for settling the debt. Both documents stress the importance of addressing financial obligations in a timely manner.
Dos and Don'ts
When filling out the Hospital Bill form, it’s essential to ensure accuracy and clarity. Here’s a list of dos and don’ts to guide you through the process:
- Do double-check all personal information for accuracy.
- Do provide complete insurance details, including policyholder information.
- Do sign the form if you are paying by credit card.
- Do make sure to include the correct amount due.
- Do keep a copy of the completed form for your records.
- Don’t leave any required fields blank.
- Don’t forget to check the box if your address or insurance information has changed.
- Don’t use a credit card without filling out the payment section.
- Don’t ignore the due date; payments are due upon receipt.
- Don’t send cash through the mail.
By following these guidelines, you can ensure a smooth and efficient billing process. Your attention to detail matters!
Key takeaways
When filling out and using the Hospital Bill form, keep these key takeaways in mind:
- Payment Details: Ensure checks are made payable to the correct entity and include the full address for remittance.
- Timely Payment: Payment is due upon receipt, so don’t delay in sending your payment to avoid any late fees.
- Contact Information: If you have questions or need assistance, call Patient Financial Services at the provided phone number.
- Online Payment Options: You can make payments online using credit cards like MasterCard, Visa, or Discover through the hospital's website.
- Review Charges: Take a moment to review the summary of charges included in the bill to understand what services were provided.
- Insurance Information: Update any changes to your address or insurance details directly on the form to ensure accurate billing.
- Itemized Statements: If you require a detailed breakdown of your charges, request an itemized statement from Patient Financial Services.
How to Use Hospital Bill
Completing the Hospital Bill form is essential for ensuring your payment is processed correctly. Follow these steps carefully to fill out the form accurately. Make sure to have your information handy as you go through each step.
- Begin by entering the date on the top right corner of the form.
- Fill in your name in the designated area, including your last name, first name, and middle initial.
- Provide your complete address, including street, city, state, and ZIP code.
- Enter your telephone number in the space provided.
- Indicate your marital status by checking the appropriate box.
- List your employer's name and telephone number.
- Fill in your employer's address, including city, state, and ZIP code.
- Next, provide details about your primary insurance company. Write the name, address, city, state, and ZIP code.
- Include your policyholder's ID number and group plan number for your primary insurance.
- If applicable, repeat the process for your secondary insurance company.
- Review the amount due and ensure it is correct. This should match the amount indicated on the invoice.
- If paying by credit card, fill out the card information, including card number, expiration date, and amount.
- Sign the form where indicated to authorize the payment.
- Check the box if your address or insurance information has changed, and indicate any changes on the reverse side.
- Detach the top portion of the form and return it with your payment.
After completing the form, make sure to send it to the address provided on the form. If you have any questions or need assistance, you can contact Patient Financial Services at the number listed. Prompt payment will help avoid any potential service fees or complications with your account.